
New Research on the Antidepressant-vs.-Placebo Debate
(Updated) In the 1990s, everyone was “Listening to Prozac,” after best-selling author Peter Kramer described sparkling personality transformations in patients who took the titular antidepressant drug. Then came the backlash: by the early 2000s, studies showed that Prozac and other selective serotonin reuptake inhibitors, or SSRIs, weren’t exactly miracle pills but were instead associated with suicide, especially in kids and teens. Another whiplash-inducing turn came in 2008, when a review of the research found that the drugs were actually no more effective than sugar pills, except in cases of the most severe depression.
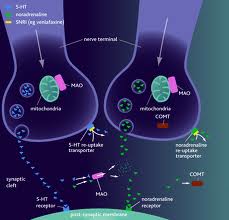
Last month, research published in the Archives of General Psychiatry sought to help explain the paradoxical findings on SSRIs and other new generation antidepressant drugs, the increasingly popular medications that are now used by more than 1 in 10 Americans over 12. Using a new statistical approach, researchers led by Dr. John Krystal at Yale University School of Medicine reanalyzed data from seven clinical trials involving 2,515 patients, whose results were used to win FDA approval for the SNRI (a drug that affects both serotonin and norepinephrine) duloxetine (Cymbalta).
Known as growth-mixture modeling, the statistical technique allowed the authors to track how individual patients improved or worsened over time in response to medication or a placebo. The researchers found that roughly three-quarters of patients did better on medication than on a placebo. “That’s much more than half and half. That’s quite favorable,” says Krystal.
However, Krystal adds, just under a quarter of patients did not respond well to drug treatment and in fact did worse on antidepressants than did patients who were given a placebo.
MORE: Report: 1 in 5 American Adults Takes Mental Health Drugs
The benefit of growth-mixture modeling is that it reveals treatment trajectories of patients rather than looking at outcomes on average. When some patients get better while others get worse, the true impact of the drug may be “canceled out” in the data if they are considered only in the aggregate, obscuring both the drug’s harms and its benefits. That may help explain why some research finds that antidepressants work no better than a placebo.
“This has enormous implications for understanding the limits of the effectiveness of our current medications,” says Krystal. “These data really caution against the demonization of antidepressants as merely placebo, but they do raise a concern that some people are better off on placebo than on the antidepressant that they’re getting.”
Irving Kirsch, professor of psychology at the University of Hull in England and author of a 2008 meta-analysis in PLoS Medicine that found little benefit of antidepressants for most patients, is less sanguine about the new study. He characterizes the results as “indeed important” but says they suggest that “while many people may benefit from antidepressant treatment (although most of them to a degree that is not clinically significant), about 1 in 4 are made worse.”
“What makes this particularly problematic is the fact that we don’t know who these people are,” Kirsch says. “Although placebo may not be a viable treatment option, there are other treatments that on average work as well as antidepressants, [such as] physical exercise and cognitive behavioral psychotherapy. As far as we know, these alternatives don’t make people worse.
“This suggests to me that antidepressants should be kept as a last resort, and if a person does not respond to the treatment within a few weeks, it should be discontinued,” says Kirsch.
Krystal agrees that if one-quarter of patients with depression are made worse by antidepressant treatment, “we need to find ways to identify who those people are and find other ways to reach that group of people.”
MORE: Study Shows Antidepressants Affect Brain Differently than Placebo
Krystal’s study also found that people who improved on a placebo did so as quickly as those who improved with medication. This is important because it suggests that using a “washout period,” a technique used in some clinical trials to weed out placebo responders by eliminating participants who respond quickly, may not work with antidepressant studies.
“It counteracts the expectations that the field has that placebo response is fast and drug response is slow. Simply having a brief placebo-exposure period is not likely to eliminate the impact of placebo on outcome,” Krystal says.
That further complicates efforts to figure out the true effects and mechanism of antidepressant drugs. “We’re going to have to study people who are worse off on drug than placebo, and [not knowing who they are] will make it harder to determine whether there’s a statistically significant effect of the drug.” And given that it may be difficult to eliminate placebo responders simply through clever study design, questions about how antidepressants work, and in whom, may not be resolved until genetic or other tests can be devised to predict individual responses.
“This going to remain a challenge for study for some time,” concludes Krystal, whose latest study was funded by the government but who has received industry funding for other research.
MORE: Study: Stress-Depression Connection Sheds Light on Antidepressant Effects
A separate study published in the American Journal of Psychiatry (AJP) in December highlights other potential complications. The authors of that paper report that since 1980, the percentage of depressed patients responding to a placebo in clinical trials has risen by 7% per decade, reaching 50% in some studies.
Why? In the early years, participants for antidepressant trials were recruited from psychiatric hospitals, which meant that only the most severe cases were included. Today, however, participants are often recruited through advertisements and are paid to be in the trials. That introduces two problems that skew study populations: the most seriously depressed people often lack the capacity even to make a phone call in response to an ad and are thus overlooked, while other people may be persuaded to exaggerate symptoms of depression in order to participate in the trials and get the money. The authors of the AJP study report cases of “professional guinea pigs” who faked symptoms or enrolled in several trials at once.
Given the complexities of studying antidepressants — which appear to be placebos for some, poisons for others and miracle pills for yet others — it seems that data analysis in antidepressant research will likely remain a growth industry for decades to come. Until scientists can work it out, patients and psychiatrists will have to try multiple methods to treat depression until they hit on something that helps, keeping in mind that antidepressant drugs may backfire for some patients.
MORE: Why American Presidents (and Some Oscar Winners) Live Longer
Correction [Jan. 23, 2012]: The original version of this story mischaracterized Cymbalta as a selective serotonin reuptake inhibitor, or SSRI. The antidepressant drug is an SNRI, which affects both norepinephrine and serotonin.
Maia Szalavitz is a health writer for TIME.com. Find her on Twitter at @maiasz. You can also continue the discussion on TIME Healthland‘s Facebook page and on Twitter at @TIMEHealthland.


Devi effettuare l'accesso per postare un commento.