 L’assassinio di Marat
L’assassinio di Marat
 Monoaniaco
Monoaniaco monomaniaca
monomaniaca Monomaniaco
Monomaniaco Pinel libera i malati di mente dalla prigione
Pinel libera i malati di mente dalla prigione Entrance Philippe Pinel (1745-1826) releasing the lunatics from their chains at the Salpêtrière Hospital in 1795.
Entrance Philippe Pinel (1745-1826) releasing the lunatics from their chains at the Salpêtrière Hospital in 1795.Nella storia della psichiatria le malattie appaiono e scompaiono come meteore. Agli inizi del secolo diciannovesimo Pinel coniò il termine mania ragionante o follia parziale , Esquirol quello di monomania omicida. Per Etienne Jean Georget allievo di Esquirol la follia parziale escludeva l’idea di azione criminale e di colpa oltre che quella di responsabilità della condotta. Il concetto originariamente autonomo di monomania, legato all’ipotesi di due differenti sedi organiche della follia l’epigastrio ed il cervello, alimentò un acceso dibattito nel corso del XIX secolo, basato su argomentazioni spesso risibili sulle quali ironizza Dostoevskij nel “ I fratelli Kamarazov”. Nel romanzo tre medici cercano di stabilire se l’imputato di omicidio fosse o meno “monomaniaco” basandosi sull’osservazione della direzione del suo sguardo all’ingresso del tribunale.
A partire dalla seconda metà dell’Ottocento prevalse l’idea che che la “follia ragionante” altro non fosse che un raggruppamento provvisorio ed artificiale di fenomeni diversi e che pertanto non si potesse considerare un’entità nosografica a se stante. Si affermò il concetto di moral insanity coniato da Prichard (1835) che si agganciava alla teoria della degenerazione di Morel e Magnan. Dopo Kraepelin i vari casi di monomania furono ascritti alle psicopatie, alla paranoia, alle psicosi organiche e dopo Eugen Bleuler alle varie forme di schizofrenia o psicopatia . La monomania scomparve perché non aveva un fondamento psicopatologico ed era facile obiettare che la psiche è un tutto in cui intelletto, affetti ed impulsi agiscono unitariamente. La monomania omicida era un concetto frutto di una visione intellettualistica e filosofica della mente umana. Le passioni e gli affetti, considerati irrazionali, per una lesione della volontà che lasciava indenne l’intelligenza avrebbero determinato l’impulso irresistibile e criminale. Non si comprendeva che poteva essere la razionalità lucida solo apparentemente integra ma in realtà anaffettiva a determinare l’agire delittuoso ed omicida.
 L’ipnotizzatore e l’isterica
L’ipnotizzatore e l’istericaAnche per l’Isteria è successo un qualcosa di analogo. A partire dal DSMIII non si trova più una categoria diagnostica riconducible al sostantivo isteria ma neppure troviamo l’aggettivo isterico sostituito da istrionico. L’istrione è il mentitore ed il commediante: l’isterico, nell’aggettivo sostantivato, diventa sinonimo di simulatore di cui il medico diffida perché può indurre in gravi errori diagnostici.
 Isterica della Salpetrière
Isterica della Salpetrière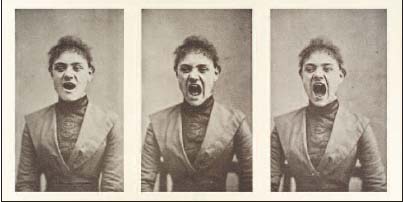 Hysterical yawnings.” Three photos in a series showing a hysterical woman screaming.
Hysterical yawnings.” Three photos in a series showing a hysterical woman screaming.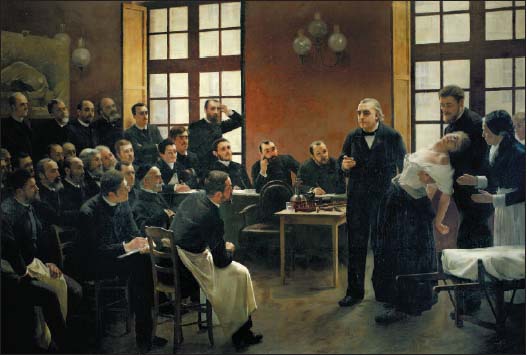 A Clinical Lesson with Doctor Charcot at the Salpêtrière.
A Clinical Lesson with Doctor Charcot at the Salpêtrière.Painting by André Brouillet, 1887. Lyon, Hôpital Neurologique. Il dipinto di André Brouillet mostra Blanche Witmann prima di una crisi. Dietro Charcot il suo famoso allievo Joseph Babinsky
Il declino dell’ Isteria ha inizio con Charcot ma anche con Breuer e Freud. Ciò che Charcot denominava isteria era una coorte composta dalle più disparate malattie. Le isteriche della Salpetrière agivano come attrici consumate abituate a mettere in scena un copione ben preciso secondo le aspettative dell’autoritario direttore. suo uso attuale il termine ‘isteria’ non ha praticamente alcun rapporto con il suo significato originario. Perché non si riferisce più a un disturbo legato all’utero od alla sessualità come si era ritenuto a partire da Ippocrate. È invece utilizzato per riferirsi a qualsiasi sintomo o qualsiasi modello di comportamento anomalo per cui non esiste patologia organica ed esso è pertanto ritenuto un prodotto di stress emotivo, ansia o qualche altra causa psicologica. Se tutti i pazienti che sembrano essere affetti da sintomi fisici, ma che non hanno alcuna patologia organica rilevabile dovessero essere soprannominati ‘isterici’, il concetto di isteria diverrebbe così ampio e così vago da essere del tutto privo di significato. Hysteria, in effetti, cessa di essere l’entità nosografica molto particolare che si è sempre storicamente considerata, e diventa semplicemente un’ affermazione negativa sulla natura di alcuni sintomi. L’aggettivo isterico ‘viene oggi utilizzato come se fosse un sinonimo di ‘non biologico’ o ‘psicogeno’.
 joseph Breuer
joseph Breuer Anna O- Bertha Pappenheim
Anna O- Bertha PappenheimQuando Breuer cominciò il trattamento di AnnaO- Bertha Pappenheim nel 1880 e fece diagnosi di Hysteria si riferiva alla natura psicogena della tosse,delle contratture, delle paralisi , dei disturbi del linguaggio e della diplopia : egli escluse per es. la possibilità di una meningite tubercolare.
E’ stato suggerito però da Mikkel Borch Jacobsen nel suo libro “Remembering Anna O. A century of mystification” (1996) che il quadro sintomatologico complessivo cui il famoso medico si trovò di fronte sia stato un’abile messa in scena attraverso la quale la giovane ebrea confermava la diagnosi di Breuer , ma fondamentalmente lo teneva in scacco. Si sarebbe trattato di una simulazione isterica od autoipnotica, che avveniva ad un livello preconscio e non di una menzogna intenzionale e pienamente cosciente. Massimo Fagioli nella sua magistrale premessa al libro “La storia di Anna O di Lucy Freeman” (L’asino d’oro” 2013) afferma che Breuer pur utilizando una volta il termine inconscio in realtà preferiva parlare di un “doppio stato di coscienza” od un’Io cattivo”: quest’ultimo potrebbe aver agito come un’abile simulatore . L’inganno riusciva perché Breuer non andava oltre i sintomi e la rievocazione dei ricordi o l’abreazione nel linguaggio degli affetti rimossi che in quanto tali erano stati un tempo coscienti. Joseph Breuer brillante neurofisiologo, rimaneva nell’ambito dell’approcio razionale alla malattia e sbagliò in partenza la diagnosi. Non collegò l’isteria alla presenza di un nucleo psicopatologico “inconscio”, nel senso di mai venuto prima alla coscienza, che si celava dietro il teatro privato della paziente ; l’anaffettività e la pulsione di annullamento non producevano manifestazioni visibili nascondendosi indisturbate dietro una teatralità vuota ed a tratti manierata.
 George Gershwin muore per un tumore cerebrale scambiato per isteria da Gregory Zilboorg
George Gershwin muore per un tumore cerebrale scambiato per isteria da Gregory ZilboorgFreud sfruttò cinicamente la malattia di AnnaO e la sua messa in scena in quanto legata alla fama ed alla credibilità di Breuer . Indusse quest’ultimo a dichiarare il falso a proposito dell’efficacia del metodo catartico nel trattamento dell’isteria per poi procedere a demolirne l’ immagine. Già nella corrispondenza con la fidanzata Freud appare particolarmente invidioso del rapporto fra Breuer ed AnnaO, che viene descritta come molto avvenente, tanto da accennare all’infelicità ed alla gelosia della moglie del collega, Mathilde. Non sappiamo quanto risponda al vero la famosa storia della gravidanza e del parto isterico di Bertha Pappeheim messa in giro dal padre della psicoanalisi : di certo è falso che Breuer concepì la figlia Dora dopo l’interruzione del trattamento e il ricovero in ospedale della giovane. Dora Breuer nacque ben tre mesi prima la fine della cura . Ciò rende inquietante un’altra comunicazione che Freud fece a Marie Bonaparte nel 1925: a causa del coinvolgimento del marito con Anna O-Bertha Pappenehim, Mathilde Breuer avrebbe tentato addirittura il suicidio durante l’allattamento della figlia Dora . Quest’ultima circostanza, se vera, testimonierebbe a favore di una grave forma di depressione .
Jacobsen, nel libro prima citato, riferisce che lo psiconalista Peter Swales ebbe modo di leggere i “Diari” di Marie Bonaparte nei quali veniva riportata una confidenza di Freud
<<Confronted by Breuer almost obsessional discussing of Anna O. all the time, his wife Mathilde made a suicide attempt. Breuer broke off the treatment. But the same night he was called back and Anna confessed to him she was pregnant by him.>>
Freud ovviamente non è attendibile sia sul piano teorico né umano per cui quanto comunicò a Marie Bonaparte va preso con beneficio di inventario: resta il fatto che l’aver scelto l’isteria come suo cavallo di battaglia può aver influito sul declino dell’isteria come entità nosografica autonoma. La psicoanalisi proprio in America dove si è più largamente diffusa nel novecento, ha invalidato la credibilità della diagnosi come ha affermato a più riprese lo psichiatra Allen Frances, il padre del DSMIII e IV. Emblematico il caso George Gerschwin. Lo storico della psichiatria , il russo Gregory Zilboorg emigrato negli USA e diventato psicoanalista freudiano con credenziali false, curava il musicista per mal di testa e anosmie ritenuti sintomi isterici ma in realtà espressione di un tumore cerebrale con esito mortale . Questo errore fa parte integrante della tradizione freudiana.
Storicamente anche Freud, del tutto in malafede aveva confuso sintomi organici con sintomi psichici . Egli, proprio nel 1895 pochi mesi prima della pubblicazione degli “Studi sull’Isteria” firmati insieme a Breuer, convinse una sua paziente isterica Emma Eckstein a sottoporsi ad un intervento al naso in base alla teoria delirante di Fliess secondo la quale la masturbazione provocava un’alterazione dei turbinati che poteva essere risolta chirurgicamente. Fliess che per la prima volta si cimentava in un’operazione del genere, lasciò mezzo metro di garza nel naso della paziente. Freud interpretava i sintomi di un’infezione che si era sviluppata come se fossero sintomi isterici. Jeffey Moussaieff Masson ha fornito un resoconto dettagliato e completo di questo episodio nel suo libro “Assalto alla verità” (1984) . La paziente costretta ad altri interventi chirurgici si salvò ma rimase per sempre sfigurata nel volto. Mentre Bertha Pappenheim- Anna O , durante la malattia, non si riconosceva allo specchio Emma Ekstein fu resa irriconoscibile. A quanto pare Freud mentre pubblicava nel 1895 gli studi in cui ribadiva la natura traumatica e psicogena dell’Isteria contemporaneamente caldeggiava l’idea che essa fosse dovuta a cause organiche dando credito all’amico berlinese, che fu a suo tempo accusato dal figlio Robert, diventato anche egli psicoanalista, di aver abusato di lui da bambino.
Quindi né Joseph Breuer nel 1880 né Freud nel 1895 avevano la minima idea di cosa fosse l’Hysteria. Breuer si trovò del tutto impreparato ad affrontare un quadro psicopatologico complesso in cui i sintomi isterici erano solo la sovrastruttura di un nucleo psicotico e dissociativo mentre Freud si limitava a ripetere le formule di Charcot sull’origine traumatica dell’isteria dedotta dall’osservazione degli effetti psichici dei primi incidenti ferroviari nell’Ottocento.
Le vicissitudini del concetto di monomania omicida e di isteria parlano di forme di razionalità diagnostica differenti. L’approccio illuministico di Pinel ed Esquirol racconta dell’illusione di una ragione integra, senza delirio che potrebbe convivere con affetti ed una volontà malate nell’impulso irresitibile dell’agire criminale. Breuer testimonia lo scacco, personalmente sofferto, di un progetto di diagnosi e cura razionale di fronte all’immagine femminile oppressa e sofferente: il caso di Anna O rappresenta un punto di crisi e un un’occasione mancata di passaggio ad una nuova psichiatria. In Freud la razionalità è strumentale piegandosi a diventare mezzo per il perseguimento di un’utile personale, la fama ed il denaro, che non rifugge ma anzi integra in sé la logica dell’agire falso e criminale che oltre a diffamare produce lesioni e morti.
 Adam Lanza imita Anders Breivik
Adam Lanza imita Anders BreivikI manuali diagnostici del terzo millenio, improntati a criteri apparentemente ateoretici ed operativi, eliminando la soggettività della valutazione medica , segnalano un’ulteriore evoluzione verso sistemi classificatori che si espandono proporzionalmente all’espansione del mercato delle case farmaceutiche . In quanto prodotto di una psichiatria disfunzionale ed acefala, che ha perso ogni riferimento alla ricerca sulla psicopatologia e sull’inconscio, essi concorrono a generare nuovi modelli di patologia mentale. Entità tradizionali come l’isteria, ma oggi anche la schizofrenia e la psicopatia, si ibridano e scavano percorsi carsici scomparendo. Quando tali entità non riconosciute riemergono alla superficie della vita sociale innescano fenomeni drammatici ed inquietanti all’interno delle quali la bizzaria dei deliri e dell’acting out criminale come nel mass shooting , si coniuga con fenomeni isterico-imitativi che contagiano una moltitudine di persone.Come scrive Allen Frances oggi
“Psychiatry is rapidly expanding and normal is shrinking”
















 American psychiatry is absolutely unable to face extremely serious psychotic situations such as Adam Lanza’s mass murdering: in this case schizophrenia hasn’t been diagnosed and aptly treated. A normal and physiological state of grief is considered pathologic and a clear psychotic state isn’t detected. The so called “mass shooting” has become almost epidemic, a sort of unconsciously repeated dramatization of the idea of a violent and hyper rational society (62.000 deaths in just a few years by firearms) that historically has been erected on racism and systematic extermination of native populations. The same war ideology that makes the United States so present in many unfair and useless conflicts, is the origin of a psychiatric emergency in the armed forces: 295 soldiers took their lives just in 2012. The only given response to this dramatic situation is a manual that’s been created with the aim of reinforcing the academic status quo, that is very far from real life and whose main interest is to obtain an economic profit for pharmaceutical sector. According to Frances the motivations that lead to the new edition of the DSM aren’t just of economic nature, tied to a very simple conflict of interests among various researchers paid by different pharmaceutical industries; this conflict, for the scientist, is a lot more of “intellectual” nature: these highly specialized researchers have the natural tendency to value their personal guidelines and ideas, to expand their sectors of study regardless of the practical clinical consequences for the unfortunate patients. It must not be underestimated that A.P.A. invested 25 millions in DSMV, and given that the previous edition has been a worldwide bestseller, a similar result is expected for this new edition as well, not only in terms of profits from the sells, but also in terms of increased popularity and prestige for the researchers – popularity and prestige that can be cashed in on as well. Even if Professor Frances’ critiques appear to be somehow well motivated, they do not decrease his personal responsibility in this announced disaster.
American psychiatry is absolutely unable to face extremely serious psychotic situations such as Adam Lanza’s mass murdering: in this case schizophrenia hasn’t been diagnosed and aptly treated. A normal and physiological state of grief is considered pathologic and a clear psychotic state isn’t detected. The so called “mass shooting” has become almost epidemic, a sort of unconsciously repeated dramatization of the idea of a violent and hyper rational society (62.000 deaths in just a few years by firearms) that historically has been erected on racism and systematic extermination of native populations. The same war ideology that makes the United States so present in many unfair and useless conflicts, is the origin of a psychiatric emergency in the armed forces: 295 soldiers took their lives just in 2012. The only given response to this dramatic situation is a manual that’s been created with the aim of reinforcing the academic status quo, that is very far from real life and whose main interest is to obtain an economic profit for pharmaceutical sector. According to Frances the motivations that lead to the new edition of the DSM aren’t just of economic nature, tied to a very simple conflict of interests among various researchers paid by different pharmaceutical industries; this conflict, for the scientist, is a lot more of “intellectual” nature: these highly specialized researchers have the natural tendency to value their personal guidelines and ideas, to expand their sectors of study regardless of the practical clinical consequences for the unfortunate patients. It must not be underestimated that A.P.A. invested 25 millions in DSMV, and given that the previous edition has been a worldwide bestseller, a similar result is expected for this new edition as well, not only in terms of profits from the sells, but also in terms of increased popularity and prestige for the researchers – popularity and prestige that can be cashed in on as well. Even if Professor Frances’ critiques appear to be somehow well motivated, they do not decrease his personal responsibility in this announced disaster.




 Adam Lanza, third from the right, posing for a group photo of the technology club which appeared in the Newtown High School yearbook
Adam Lanza, third from the right, posing for a group photo of the technology club which appeared in the Newtown High School yearbook
 (Top row from left) Charlotte Bacon, Daniel Barden, Olivia Engel, Josephine Gay, Ana Marquez-Green. (Middle row from left) Dylan Hockley, Catherine Hubbard, Chase Kowalski, Jesse Lewis, James Mattioli. (Bottom row from left) Grace McDonnell, Emilie Parker, Noah Pozner, Caroline Previdi, Jessica Rekos
(Top row from left) Charlotte Bacon, Daniel Barden, Olivia Engel, Josephine Gay, Ana Marquez-Green. (Middle row from left) Dylan Hockley, Catherine Hubbard, Chase Kowalski, Jesse Lewis, James Mattioli. (Bottom row from left) Grace McDonnell, Emilie Parker, Noah Pozner, Caroline Previdi, Jessica Rekos



{kind=link}
Devi effettuare l'accesso per postare un commento.