

Bioetica disumana. L’aborto postnatale
Uccidere un neonato non è come fare un’interruzione di gravidanza. Ecco perché è inaccettabile la proposta avanzata in un ciclo di conferenze nelle università italiane, da Alberto Giubilini e Francesca Minerva dell’università di Melbourne
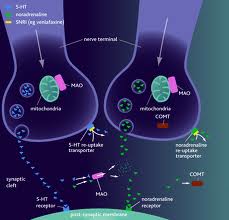
Lo sviluppo della medicina moderna legata alle tecnologie biomediche costituisce una sfida alle tradizionali concezioni razionali e religiose dell’uomo. Le scoperte dell’embriologia e delle neuroscienze hanno aperto una nuova visione dell’ontogenesi, cioè dello sviluppo biologico, che ha radicalmente cambiato anche la nostra concezione della nascita umana. Nessuno attualmente può ignorare che il cervello fetale ha una funzione dei neurotrasmettitori sostanzialmente diversa da quello neonatale. Ciò comporta che il feto, contrariamente al neonato, non prova dolore. Nessuno inoltre può continuare ad ignorare che alla nascita lo stimolo luminoso attiva dei geni ad azione immediata che modificano in toto la fisiologia cerebrale, facendo emergere capacità di pensiero come affermato dalla Teoria della nascita di Massimo Fagioli, inesistenti in utero. Queste conoscenze scientifiche sono il risultato di una ricerca sperimentale che non può essere negata come si faceva ai tempi in cui le dissezioni anatomiche venivano proibite subordinando la biologia alla religione. L’etica astratta del pensiero religioso si opponeva al progresso della conoscenza medica come, a suo tempo, si era opposta alla scienza fisica.Oggi quindi stupisce che un gruppo di filosofi in nome dei valori della bioetica vadano in giro per le università italiane dissertando se il bambino, una volta fuori dall’utero, sia o meno “persona”. Partecipando ad un congresso di bioetica dedicato alla nascita ed alle relative terapie intensive potrebbe accadere che il grande assente sia proprio il neonato nella sua realtà biologica e psichica di cui si fa finta di parlare ma che viene completamente annullato.
Può anche accadere che in talune congreghe di filosofi riunite per affinità ideologiche, si sostenga che il feto è uguale al neonato: se è pertanto legittimo l’aborto fetale lo sarebbe altrettanto il cosiddetto aborto neonatale. Questi esiti paradossali della logica razionale non devono sorprendere. Partendo dalla premessa che la nascita sia solo una parola alla quale non corrisponde nessuna cesura o trasformazione sul piano biologico e psichico, si giunge sia alla conclusione della sacralità del concepito, già “persona fin dallo zigote per i cattolici, in barba ad ogni principio di genetica, sia all’affermazione, da parte dei bioeticisti laici, della assoluta disponibilità della vita del neonato. Siccome quest’ultimo non avrebbe nessuna coscienza di sé esso potrebbe essere tranquillamente soppresso qualora la sua sopravvivenza urtasse con gli interessi della madre. La bioetica cosiddetta laico-utilitaristica, con la tesi di Minerva e Giubilini sull’aborto postnatale, si avvicina pericolosamente alla logica nazista dalla quale pretende di aver preso le distanze a partire dalla dichiarazione dei diritti dell’uomo nel 1948 e dalla condanna della eliminazione delle vite ritenute inutili dal Terzo Reich. Bioeticisti laici e cattolici su una cosa sono d’accordo: sul fatto che la medicina si troverebbe in una condizione di minorità intellettuale e morale necessitando di qualcuno che le chiarisca cos’è la vita umana e la morte umana facendo ricorso alla ragione: quest’ultima, da Platone ed Aristotele fino ai giorni nostri, su questi temi ha sostenuto tutto ed il contrario di tutto. Ha sostenuto per esempio che la donna ed il bambino non sono esseri umani in quanto sprovvisti della ragione. L’altra grande imputata è la tecnologia medica sospetta di poter generare delle mostruosità e di essere incline ad un delirio di onnipotenza e dominio totale esercitato da uomini su altri uomini. Addirittura nel tentativo di screditare la ricerca biologica alcuni si spingono fino a fornire una falsa interpretazione storica della genesi del pensiero medico a partire dalla figura leggendaria di Ippocrate. Si dice, operando una indebita semplificazione e proponendo una ricostruzione riduttiva e parziale, che il discendente di Asclepio avrebbe sostenuto la sacralità della vita in linea con la concezione cattolica attuale. Bisogna ricordare che nel giuramento di Ippocrate è contenuto il principio del non accanimento terapeutico. NelDe morbo sacro che fa parte degli scritti ippocratici si sostiene inoltre che la malattia non ha un’origine divina ma è dovuta a cause naturali individuabili attraverso l’esame clinico. La medicina greca anticipa il metodo di indagine e le forme della razionalità scientifica essendo basata sull’osservazione empirica. Oggi assistiamo al processo per il quale la religione cattolica, forte dei suoi dogmi, e la filosofia con il suo razionalismo laico, vogliono dare dei suggerimenti alla medicina che viene accusata di avere una visione riduttiva dell’essere umano concepito solo come un insieme di meccanismi biologici. Ora il riduzionismo, che è una forma di estremismo, può essere considerato una malattia infantile della biologia. Nessun ricercatore nell’ambito delle neuroscienze sosterrebbe ai giorni nostri le tesi della prima generazione di neuroscienziati, che forti di alcune loro scoperte pretendevano di dire cosa fosse l’uomo o la malattia mentale, partendo da semplici molecole o da meccanismi neuronali elementari.
Il medico oggi che è impegnato nella ricerca sulla realtà umana deve avere la consapevolezza dei procedimenti metodologici che utilizza nel produrre le proprie conoscenze. Questa consapevolezza è parte integrante ed imprescindibile del suo bagaglio culturale. Nessuno potrebbe attualmente svolgere un’indagine scientifica sull’ontogenesi umana con una mentalità positivistica, come ai tempi di Claude Bernard, prescindendo dalla conoscenza dei processi psichici, coscienti e non coscienti che è possibile individuare soltanto facendo riferimento al rapporto fra gli individui che inizia a partire dalla nascita. I neonatologi, che accuratamente i bioeticisti escludono dai loro congressi, non si occupano solo di fisiologia o patologia del corpo, come si vorrebbe far credere, ma rivolgono la loro attenzione alla globalità psicofisica del bambino che venuto alla luce, comincia a fare esperienza di sé e del mondo. Se vogliamo cogliere un’etica nell’agire della medicina essa coincide con la ricerca e l’affermazione della verità relativa alla realtà umana. La verità del neonato, così come la si apprende dalla frequentazione della sala parto e non da solipsistiche meditazioni dietro una scrivania, è nel suo essere un soggetto pensante ed in relazione con il mondo nella sua globalità fin dai primi istanti di vita. A questa conclusione si giunge non solo attraverso l’interpretazione degli esami strumentali che sono in grado oggi di mostrarci in tempo reale le modificazioni del il funzionamento cerebrale ma anche attraverso l’interazione diretta con il bambino che, in accordo con la ricerca psichiatrica, suggerisce la presenza di una interiorità originaria fatta di fantasia, affetti e pulsioni senza parola: nel neonato è presente quel pensiero irrazionale, che si manifesta ogni notte nella creazione dei nostri sogni, come dice lo psichiatra Massimo Fagioli. Quest’ultimo,
con la sua prassi terapeutica pluridecennale ha dimostrato che le immagini oniriche sono un linguaggio dotato di senso. Al contrario il cattolicesimo aveva storicamente condannato i sogni come manifestazione demoniaca mentre Freud aveva voluto vedere in essi solo l’espressione della psicosi e della dissociazione. Freud razionalista e laico era in perfetta sintonia ed accordo con il cattolicesimo nel concettualizzare non solo una colpa o perversione originaria ma anche una totale irrilevanza della nascita come momento costitutivo della vita umana: egli come i cattolici, non riusciva a pensare ad una trasformazione conseguente alla cesura radicale fra stato fetale e stato neonatale nell’atto di venire alla luce. Stupisce nei filosofi bioeticisti laici e cattolici proprio l’ignoranza della ricerca biologica che essi pretenderebbero di regolamentare. Stupisce anche il fatto che dalla storia passata, dalle vicende della cultura del Novecento, che ha visto prosperare la complicità fra le ideologie razionali e la fede nel negare la realtà umana della nascita, non si sia appreso nulla come se ciascuno di noi dovesse essere condannato ad una eterna ripetizione di idee false e superate.











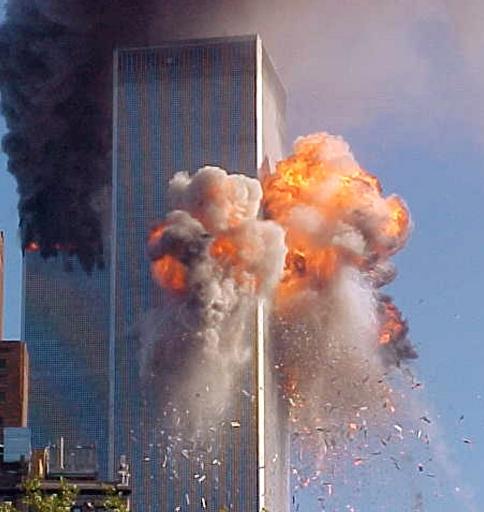
 American psychiatry is absolutely unable to face extremely serious psychotic situations such as Adam Lanza’s mass murdering: in this case schizophrenia hasn’t been diagnosed and aptly treated. A normal and physiological state of grief is considered pathologic and a clear psychotic state isn’t detected. The so called “mass shooting” has become almost epidemic, a sort of unconsciously repeated dramatization of the idea of a violent and hyper rational society (62.000 deaths in just a few years by firearms) that historically has been erected on racism and systematic extermination of native populations. The same war ideology that makes the United States so present in many unfair and useless conflicts, is the origin of a psychiatric emergency in the armed forces: 295 soldiers took their lives just in 2012. The only given response to this dramatic situation is a manual that’s been created with the aim of reinforcing the academic status quo, that is very far from real life and whose main interest is to obtain an economic profit for pharmaceutical sector. According to Frances the motivations that lead to the new edition of the DSM aren’t just of economic nature, tied to a very simple conflict of interests among various researchers paid by different pharmaceutical industries; this conflict, for the scientist, is a lot more of “intellectual” nature: these highly specialized researchers have the natural tendency to value their personal guidelines and ideas, to expand their sectors of study regardless of the practical clinical consequences for the unfortunate patients. It must not be underestimated that A.P.A. invested 25 millions in DSMV, and given that the previous edition has been a worldwide bestseller, a similar result is expected for this new edition as well, not only in terms of profits from the sells, but also in terms of increased popularity and prestige for the researchers – popularity and prestige that can be cashed in on as well. Even if Professor Frances’ critiques appear to be somehow well motivated, they do not decrease his personal responsibility in this announced disaster.
American psychiatry is absolutely unable to face extremely serious psychotic situations such as Adam Lanza’s mass murdering: in this case schizophrenia hasn’t been diagnosed and aptly treated. A normal and physiological state of grief is considered pathologic and a clear psychotic state isn’t detected. The so called “mass shooting” has become almost epidemic, a sort of unconsciously repeated dramatization of the idea of a violent and hyper rational society (62.000 deaths in just a few years by firearms) that historically has been erected on racism and systematic extermination of native populations. The same war ideology that makes the United States so present in many unfair and useless conflicts, is the origin of a psychiatric emergency in the armed forces: 295 soldiers took their lives just in 2012. The only given response to this dramatic situation is a manual that’s been created with the aim of reinforcing the academic status quo, that is very far from real life and whose main interest is to obtain an economic profit for pharmaceutical sector. According to Frances the motivations that lead to the new edition of the DSM aren’t just of economic nature, tied to a very simple conflict of interests among various researchers paid by different pharmaceutical industries; this conflict, for the scientist, is a lot more of “intellectual” nature: these highly specialized researchers have the natural tendency to value their personal guidelines and ideas, to expand their sectors of study regardless of the practical clinical consequences for the unfortunate patients. It must not be underestimated that A.P.A. invested 25 millions in DSMV, and given that the previous edition has been a worldwide bestseller, a similar result is expected for this new edition as well, not only in terms of profits from the sells, but also in terms of increased popularity and prestige for the researchers – popularity and prestige that can be cashed in on as well. Even if Professor Frances’ critiques appear to be somehow well motivated, they do not decrease his personal responsibility in this announced disaster.





Devi effettuare l'accesso per postare un commento.