 Neuroleptic Drugs and Violence
Neuroleptic Drugs and Violence
Catherine Clarke SRN, SCM, MSSCH, MBChA.
and Jan Evans MCSP. Grad Dip Phys.
August 19th, 2012
Introduction
We address the fact that the treatment for Severe Mental Illness (SMI) is neuroleptic medication. One has to give significant thought about the involvement of neuroleptic medications with the tragic circumstances of individuals who have perpetuated a progressive catalogue of catastrophic actions, and the many victims and their families who so sadly are caught up in such tragedies.
It is established that there is an increased risk of violence by people with a mental health diagnosis. A greater risk of violent behaviour (27.6%) has been found for patients who commit substance abuse, compared to non-abusers (8.5%). For patients with schizophrenia, 13.2 % committed at least one violent offence, compared with 5.3% of the general population.1
Violence is reported with command hallucinations: 48% experienced harmful or dangerous actions and this increased to 63% in medium secure units and was significantly higher, 83%, in the forensic population.2
People who are classified as SMI i.e. with schizophrenia or bipolar often experience violent incidents following a diagnosis of SMI, even though they don’t consume alcohol or use street drugs, nor having a past history of violence or command hallucinations to harm others.
Our purpose of this document is to provide a referenced explanation of how neuroleptic medications are a potential cause of violence. We take a physiological perspective concerning pharmacogenetic variants and the disruption of neurotransmitters. In Part 1 we discuss what is known about Neuroleptics and Neurotransmitters; in Part 2, the Neuroleptic Disruption of Neurotransmitters
Part 1
The first part of this document has the following structure:
· Violence
- Neuroleptic Adverse Effects on Behaviour
- Serotonin Disruption
- Noradrenaline/Norepinephrine Disruption
- Acetylcholine Disruption including Neuroleptic Malignant Syndrome and Organophosphate Poisoning
· Neuroleptic Withdrawal Adverse Effects on Behaviour
· Neurotransmitter Functioning and Behaviour
· Increased Prescribing of Neuroleptics as a Risk for Increased Violence
Violence
This is an important issue. In three acute psychiatric units in Australia it was reported: “58 % of the incidents were serious violent incidents.”3 In an attempt to address psychiatric violence in the UK, the National Institute for Health and Clinical Excellence (NICE) has a full clinical guideline: Violence. The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments.4 Although this addresses many issues, it omits the following potential causes of violence:
- Neuroleptic medications – due to neuroleptic disruption of neurotransmitter circuits such as dopamine, serotonin, norepinephrine/noradrenaline and acetylcholine.
- Pharmacogenetics – the issue of inefficient neuroleptic metabolising.
Adverse Effects on Behaviour of Neuroleptics
Neuroleptic toxic adverse reactions are related to behavioural changes such as akathesia, which is known to be a predisposing factor to violence5 and was formally recognised in the late 1970s.6
The symptoms of akathisia, an extreme, involuntary internal physical and emotional restlessness, includes restlessness, agitation and irritability.
When there is an existing precondition of akathisia, any perceived untoward disrespectful attitudes or verbal communications can trigger violence. When patients are agitated or irritable, they are less able to cope with perceived disrespect and are more prone to respond violently.
A marked increase of violence has occurred with patients prescribed moderately high-doses of haloperidol,7 and with Asian patients clozapine played a role in causing aggression and disruptive behaviour.8 Both the older ‘typical’ and the newer ‘atypical’ neuroleptics are associated with adverse behavioural reactions in a study reporting that “the newer antipsychotics did not reduce violence more than perphenazine.”9
Chart Depicting Toxic Behavioural Effects for Typical Neuroleptics:
|
Typical Neuroleptics
|
Adverse Reactions Related to Violence
|
| Clopixol |
Agitation & akathisia |
| Haloperidol |
Restlessness, agitation and violence |
| Stelazine |
Restlessness |
| Sulpiride |
Restlessness & akathisia |
Refs 7, 10 &11
Chart Depicting the Toxic Behavioural Effects for Atypical Neuroleptics:
|
Atypical Neuroleptics |
Adverse Reactions Related to Violence |
| Abilify |
Restlessness, agitation and akathisia |
| Amisulpride |
Agitation |
Clozaril
|
Akathisia and agitation |
| Olanzapine |
Restlessness and agitation |
| Palperidone/Invega |
Akathisia and aggression |
| Quetiapine |
Akathisia and irritability |
| Risperidone |
Agitation |
| Sertindole |
Akathisia |
| Zotepine |
Akathisia |
Ref 10
Observations in prison have also associated neuroleptic treatment with increased aggressive behaviour. Inmates were better able to control their aggression until they were prescribed neuroleptics and then the aggression rate almost tripled.12
Neuroleptic Withdrawal Adverse Effects on Behaviour
There is also the issue of violence experienced during withdrawal. Irritability and agitation is reported in association with neuroleptic withdrawal,13 and a direct reference links akathisia following the withdrawal of a depot in an inpatient setting.14 Irritability, agitation and akathisia need to be recognised as reactions to neuroleptic withdrawal.
In order to prevent violence in association with akathisia and withdrawal, this process needs to be undertaken by a professional or lay-person who understands the potential problems and can therefore guard against unwittingly appearing at all antagonistic to the patient.
Neurotransmitter Functioning and Behaviour
Fundamentally, human behaviour is determined by neurotransmitter functioning and “A rich literature exists to support the notion that monoamine (i.e. serotonin, dopamine, and norepinephrine) neurotransmitter functioning is related to human aggressive behaviour.”15
Dopamine, serotonin and all other neurotransmitter circuits are interdependent and any disturbance in one will result in an imbalance in them all, disrupting normal functioning. Jackson’s First Law of Biopsychiatry states: “For every action, there is an unequal and frequently unpredictable reaction.”16
Chronic neuroleptic treatment causes unpredictable behavioural reactions due to dysregulation and disruptions between dopamine, serotonin and acetylcholine neurotransmitters.
Neuroleptics and Serotonin Disruption
Some neuroleptics are known as serotomimetic drugs, affecting serotonin receptors – some block the receptors and some make them more active. “There are 14 different types of serotonin receptors that may be targeted by neuroleptics, with risperidone, clozapine, olanzapine, quetiapine and clopixol especially affecting the serotonin 5-HT2 receptor.”17
Mental status changes occur in Serotonin Syndrome. This is caused by neuroleptic drugs due to serotonin toxicity.
Animal research indicates that serotonin disruption is associated with increased violence. Reduced levels of a specific serotonin metabolite (5-HIAA) in cerebrospinal fluid has been linked with increased aggression in both dogs and male rhesus macaques18-19 and low concentrations of 5-HIAA in different cultures have been consistently reported to be associated with impulsive destructive behaviours, aggression and violence.20
Since “Impulsive violence is closely linked to serotonergic function and to several brain regions”21 and since impulsivity is also linked with both low and high serotonin levels it is difficult to know which of these changes play the most important role in treatment emergent violence.”17
The reciprocal interaction between the dopaminergic and serotonergic systems disturbed by either dopaminergic blockers or serotonergic enhancers leads to the disruption of homeostasis.22 Although the serotonin system and its interactions with other neurotransmitters are complex and full information is difficult to find, there are clear research papers, which show that serotonin and aggression are related.
Chart depicting Neuroleptic Serotonin Disruption associated Adverse Toxic Behavioural Effects:
| Akathisia |
Irritability |
| Suicidality |
Violence
|
| Arson |
Aggression |
| Violent Crime |
Self Destructiveness |
| Impulsive Acts |
Agitation |
| Hostility |
Violent Suicide |
| Argumentativeness |
|
Ref 23 & 24
Neuroleptics and Noradrenaline/Norepinephrine Disruption
Neuroleptics affect the norepinephrine neurotransmitter and akathisia induction with haloperidol is known to be associated with increased noradrenaline turnover.25- 26
Neuroleptics and Acetylcholine Disruption
An important function of the acetylcholine neurotransmitter is the control of psychological defence mechanisms including fight or flight responses. Such responses are impulsive and naturally include aggression and violence.
In varying degrees, all neuroleptic drugs have anticholinergic properties. This means that they block and cause disruption to the acetylcholine neurotransmitters. The body compensates and responds by making and releasing more acetylcholine.27
Acetylcholine Disruption and Increased Violence
Aggressive responses such as defensive rage and violence have been linked with excessive acetylcholine in animals28 –30 and a relative acetylcholine increase is associated with neuroleptic drugs due to the disruption of the dopamine-acetylcholine equilibrium.31-32
Since excessive acetylcholine is linked with aggression and violence in animals, it is likely that neuroleptic induced acetylcholine abundance triggers aggression and violence in humans.
Neuroleptic → Disrupted dopamine-acetylcholine equilibrium → Relative acetylcholine increase → Aggression/Violence.
Neuroleptic Malignant Syndrome and Organophosphate Exposure
Neuroleptic Malignant Syndrome (NMS) is an adverse effect of neuroleptics, a potentially fatal condition with up to 76% mortality rate. Symptoms of NMS include aggression, agitation and violence.27 & 33 New research associates NMS with elevated acetylcholine.34
Organophosphate chemicals form the basis of many insecticides, herbicides and nerve gases. They block the action of the body’s acetylcholinesterase enzyme, which breaks down acetylcholine so it may be processed and recycled. Excessive acetylcholine accumulates in the nervous system if the action of this enzyme is blocked.
Prolonged and repeated exposure to Organophosphates results in Chronic Organophosphate-Induced Neuropsychiatric Disorder (COPIND) e.g. in farmers who handle pesticides, due to chronic Organophosphate Poisoning (OP). COPIND behavioural symptom changes include: Hostility, Anger, Aggression and Violence.35-36 Since OP results in excessive acetylcholine, which is linked with aggression and violence in animals, the behavioural changes in COPIND are highly likely caused by excessive acetylcholine.
The link between Neuroleptic Malignant Syndrome and Organophosphate Poisoning
The symptoms of NMS and OP are similar. In both NMS and OP the replication of symptoms is due to autonomic instability and stems from disruption of the acetylcholine circuits and transmitters of the Autonomic Nervous System, involved with vital involuntary functions.
Autonomic Instability includes profuse sweating, high blood pressure, low blood pressure, respiratory distress, drooling, urinary or faecal incontinence, increased and
decreased heart rate.27
Chart Depicting the Symptom Similarities of NMS and OP
|
Neuroleptic Malignant Syndrome |
Organophosphate Poisoning
|
| Autonomic nervous system disturbance |
Autonomic Instability |
Aggression, agitation and violence
|
Aggression |
| Muscle rigidity |
Paralysis, Dystonia, Cranial nerve palsy and polyneuropathy |
| Muscle breakdown |
Weak respiratory and limb muscles |
| Coma, alterations of consciousness |
Loss of consciousness |
| Confusion |
Dementia, psychosis, anxiety, depression |
| Fever |
Seizures |
Refs 27 & 33
Conclusion: Organophosphates, Neuroleptics and Violence
Organophosphate Poisoning results in over stimulated acetylcholine neuro-circuits and systems. The action of neuroleptics is similar. It is generally accepted that Organophosphate Poisoning results in behavioural changes including violence.
Despite research to show that neuroleptics are associated with disrupted acetylcholine, it is not yet generally accepted that neuroleptics are a potential cause of violence.
Antipsychotic/neuroleptic drugs have strong anti-cholinergic properties and long-term use causes behavioural changes, which replicate the same behavioural changes occurring in chronic Organophosphate Poisoning:
“This adaptation (to psychiatric drugs – author input) replicates the effect of organophosphate poisoning whether by nerve gas, by insecticide, or by anti-Alzheimers pharmaceuticals by over stimulating acetylcholine circuits of the brain.”27
Increased Prescribing of Neuroleptics
There has been a distinct increase in neuroleptic medications, prescribed as part of treatment for mental health issues.
In the UK between 1998 and 2010, Neuroleptic drug prescriptions increased by an average of 5.1% every year.37 Over twelve years, this is a total increase of 60%.
In England, the approximate number of neuroleptic and depot (injection) prescriptions used by outpatients:
2008 – 7.0 million
2009 – 7.3 million
2010 – 7.6 million
2011 – 7.9 million38
However, due to confidentiality, the data for the number of neuroleptic prescriptions in inpatient settings is not made available. So the actual total increase of neuroleptic prescriptions in the UK is unknown.
Increased Prescribing as a Risk for Increased Violence
As outlined above, neuroleptics are a possible cause of violence. With ever increased prescribing of neuroleptic medications, it is reasonable to expect an increased amount of violent behaviour amongst those with a severe mental health diagnosis.
Since neuroleptic prescriptions are increasing by 300,000 per year in the UK, it is hypothesized that the rise in violence for neuroleptic-treated patients will escalate, whether in the community or in acute wards, secure units, prisons or outpatient units.
Part 2. Neuroleptics and Pharmacogenetics
The second part of this document has the following structure:
- Introduction to Pharmacogenetics regarding Neuroleptics
- Pharmacogenetics and Ethnic Black Populations
- Black Populations and Psychiatric Intensive Care Units
- Black Populations, detention under the UK Mental Health Act and UK Community Treatment Orders
- Pharmacogenetics as an explanation for Black Over-representation in
Psychiatric Intensive Care Units, detentions within the UK Mental
Health Act and Community Treatment Orders
Introduction to Pharmacogenetics with regards to Neuroleptics
Pharmacogenetics is the science of how drugs are broken down and used – i.e. metabolised in the body, mainly in the liver, by the genetically diverse Cytochrome P450 (CYP450) enzyme system and other drug metabolising systems. There are many CYP450 variants that affect therapeutic efficacy and inefficacy of medications.
Extensive Metabolisers are efficient metabolisers, whereby side-effects do not build up. Poor Metabolisers are inefficient metabolisers that have no metabolising activity whatsoever; this means that drug toxicities do build up and cause side effects. Intermediate Metabolisers have approximately 50% drug metabolising capacity and produce lesser side-effects than Poor Metabolisers.39 Ultra Rapid Metabolisers/ Hyperinducers have higher than normal rates of drug metabolism; Those medications which are classified as prodrugs are inactive until metabolised in the body, therefore Ultra Rapid Metabolisers are at increased risk of drug-induced side effects due to increased exposure to prodrug active drug metabolites.40
Neuroleptic drugs are metabolised through CYP450 enzymes e.g.CYP450 1A2, 2D6 and 2C19. A single neuroleptic can necessitate a combination of CYP450 enzymes for metabolisation.
All SMI patients who are Poor and/or Intermediate Metabolisers of neuroleptics, and Ultra Metabolisers of neuroleptic prodrugs; e.g. paliperidone, the active metabolite of risperidone; will inevitably suffer neurological and behavioural changes due to toxicities incurred from the inability to metabolise neuroleptics efficiently. Polypharmacy compounds the toxicities.
CYP450 1A2 Metabolising Pathway and Neuroleptics
CYP450 1A2 enzyme pathway has many variants and metabolises olanzapine and haloperidol and is the major metabolising enzyme for clozapine.
CYP1A2*1C and *1D Poor Metabolisers have been associated with increased clozapine exposure and adverse reactions.41 CYP1A2*1K is also Poor Metaboliser genotype.42
In one study, Asian patients who were prescribed clozapine, experienced aggression and disruptive behaviour who, following clozapine discontinuation, had marked improvement.8 The genotype of the Asian patients in the study is unknown, however since 25% of Asians have CYP1A2*1C Poor Metaboliser genotype,43 it is possible these patients were either CYP1A2*1C, *1D or *1K or a combination of these Poor Metaboliser genotypes.
Additionally15-20% of Asians are Poor Metabolisers for CYP2C19 and 2% are Poor Metabolisers for CYP2D6.44CYP2C19 and CYP2D6 metabolise clozapine as well as CYP1A2; any of these combinations are possible and could have predisposed to disruptive behaviour.
CYP450 2D6 Metabolising Pathway and Neuroleptics
75% of all psychotropic drugs, including neuroleptics, are metabolised via CYP450 2D6.45 CYP450 2D6 is a highly variable enzyme with a significant percentage of the population being Poor, Intermediate or Ultra Metabolisers and is linked with a poor therapeutic response and adverse reactions.
Violence in relation with serotonin toxicity/akathisia has been linked with pharmacogenetic CYP450 2D6 drug metabolising variants.46
Pharmacogenetics and Ethnic Black Populations
Due to genetic variations there is higher incidence of Poor Metaboliser and Ultra Metaboliser status in Black populations, compared with White and Asian populations for the CYP 450 2D6 pathway. “The prevalence of poor metabolizers in Black populations has been estimated from 0 to 19%, compared with consistent reports of poor metabolizer status in Caucasians (5–10%) and Asians (0–2%).”47
Recalling that 75% of neuroleptic medications are metabolised via CYP450 2D6, the following table shows the variation of metabolising ability in black ethnic populations for CYP450 2D6.
| |
Poor Metabolisers
|
Ultra Metabolisers
|
|
| South Africans |
18.8%
|
|
| Nigerians |
8.6-8.3%
|
|
| Ghanaians |
6%
|
|
| African – American |
3.9%
|
2.4%
|
| Zimbabwean |
2%
|
|
| Tanzanian |
2%
|
|
| American Black |
1.9%
|
|
| Ethiopians |
1.8%
|
29%
|
Ref 48
29% of Ethiopians and 2.4% of North African Americans are Ultra Metabolisers via CYP450 2D6 pathway.48 Furthermore, 10-20% of Africans are Poor Metabolisers and 5% are Ultra Metabolisers via CYP450 2C19.49
Many prescription medications can lead to “serious mental change.”50 Since black populations statistically have difficulty in metabolising general and psychotropic medications and cannabis via the CYP450 pathways, this factor could contribute to BME groups living in the UK who are more likely to be diagnosed with a Mental Health problem and admitted to hospital.51
Psychiatric Intensive Care Units and Over-representation of Black Populations
In UK Psychiatric Intensive Care Units (PICU), there is clear over-representation of black ethnic patients.52 Another study showed fifty-five percent of PICU admissions came from ethnic minorities(compared with 25.6% of total hospital admissions and 20.9%of the local catchment area population aged between 16 and 65years).53
“TypicalPICU patients are male, younger, single, unemployed, sufferingfrom schizophrenia or mania, from a Black Caribbean or Africanbackground, legally detained, with a forensic history. The mostcommon reason for admission is for aggression management.”54
UK Mental Health Act Detentions and Over-representation of Black Populations
There is also a disproportionately large representation of Black Minority and Ethnic (BME) origin when considering those who are legally detained under the UK Mental Health Act.
The proportion of black and black British people legally detained rose by 9.7%, with a 9% rise in the number of Asian or Asian British and mixed-race people detained for treatment, compared to a 0.3% rise for the overall number of people detained from 2007/8 to 2008/9. This disparity grew and 53.9% of black/black British inpatients spent time compulsorily detained, as did almost half of mixed-race inpatients and over 40% of Asian/Asian British inpatients, compared with 31.8% of all psychiatric inpatients who spent some time detained during the year.55
UK Community Treatment Orders and Black Populations
Legal UK Community Treatment Orders are enforced when patients have received mental health ‘treatment’ i.e. neuroleptics and history of violence; BME Groups have more Community Treatment Orders than white populations.56
“There is a possible relationship for psychiatric in-patients between compulsory detention, disturbed behaviour, depot medication and being black, which is not satisfactorily explained by diagnosis alone.”57
The higher incidence of mental health problems in black populations is most likely due to the higher incidence of Poor, Intermediate and Ultra Metabolisers and the associated problems with metabolising medications.
Synopsis
Neuroleptics can be a cause of violence due to neurotransmitter disruption.
Violence must be considered not simply as an indication of how deeply schizophrenia /bipolar illness can worsen, but as an adverse effect of neuroleptic treatment.
People who are inefficient metabolisers are likely to suffer more severe adverse effects and become violent or aggressive.
BME populations have a higher incidence of inefficient metabolisers and as such a higher incidence of violence leading to PICU admissions and Mental Health Act detentions.
However whatever the nationality, when individuals are Poor and Intermediate Metabolisers and Ultra Rapid Metabolisers for prodrugs, the impact of neuroleptics in triggering akathisia, aggression or irritability can trigger violence indiscriminately.
Conclusion
There is a larger incidence of violence in people with a severe mental health diagnosis than in the general population. The severely mentally ill are invariably treated with neuroleptic medication which itself can be the cause of violence since neuroleptic medications disrupt neurotransmitter functions. This disruption of neurotransmitter functioning can precipitate violent behaviour. Withdrawal of neuroleptic medication – due again to the disruption of neurotransmitters – is also associated with violence.
Pharmacogenetics show that the some people are unable to metabolise neuroleptic medication and this inability can result in further disruption of neurotransmitter functioning with a likelihood of increased violence.
The inability to metabolise neuroleptic medication is particularly prevalent in BME populations. As a consequence this population experience more violence which is confirmed in practice by an over representation of BME individuals, both on Psychiatric Intensive Care Units (PICUs) where a common reason for admission is aggression, and the use of Mental Health Act detentions and Community Treatment Orders.
With the trend towards increased prescribing of neuroleptic medications, a level of increased violence can be anticipated for the future.
There is the possibility of ameliorating the presence of violence in the severely mentally ill by ensuring pharmacogenetics is more fully recognised as a significant factor, and that genotype testing is adopted in order to assess the ability of the individual to metabolise neuroleptic medication. Without this testing,
much of the violence in psychiatry can be laid at the door of psychiatrists and the pharmaceutical companies.
References:
Ref 1 Fazel S, et al, (2009) http://www.ncbi.nlm.nih.gov/pubmed/19454640
Ref 2 Birchwood et al. (2011)
http://www.biomedcentral.com/1471-244X/11/155/
Ref 3 Owen C. et al, (1998) http://ps.psychiatryonline.org/article.aspx?Volume=49&page=1452&journalID=18
Ref 4 http://www.nice.org.uk/nicemedia/live/10964/29715/29715.pdf
Ref 5 Crowner ML, et al (1990) http://www.ncbi.nlm.nih.gov/pubmed/1973544
Ref 6 GB. Leong, M.D. and JA Silva, M.D. (2003)
http://library-resources.cqu.edu.au/JFS/PDF/vol_48/iss_1/JFS2002173_481.pdf
Ref 7 John N. Herrera et al (1998)
http://psychrights.org/research/Digest/NLPs/RWhitakerAffidavit/HerreraNeurolepticsandViolence.PDF
Ref 8 KA.Mansour, C.Willan and J.Follansbee (2003) http://bapauk.com/doc/Deteriorationofpsychosisinducedbyclozapine_41.doc
Ref 9 Jeffrey W. Swanson et al, (2008) http://bjp.rcpsych.org/content/193/1/37.full
Ref 10 Drug Monographs, Prescribing information and UK NICE Guidelines 2007 – 2012.
Ref 11 Jerome L. Schulte, (1985) http://psychrights.org/research/Digest/NLPs/RWhitakerAffidavit/Schulte.PDF
Ref 12 D.G. Workman and D.G. Cunningham (1975) page 65
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2274756/pdf/canfamphys00332-0065.pdf
Ref 13 MIND http://www.mind.org.uk/help/medical_and_alternative_care/making_sense_of_coming_off_psychiatric_drugs
Ref 14 Theodore Van Putten, (1975)
http://psychrights.org/research/Digest/NLPs/RWhitakerAffidavit/VanPuttenManyFacesofAkathisia.PDF
Ref 15 Berman ME, Coccaro EF. “Neurobiologic correlates of violence: relevance to
criminal responsibility.” Behav Sci Law. 1998 Summer;16(3):303-18. Review.
http://www.ncbi.nlm.nih.gov/pubmed/9768463
Ref16 Jackson, Grace E. MD, Appendix D, Transcript of
“What Doctors May Not Tell You About Psychiatric Drugs”
Public Lecture, Centre for Community Mental Health – UCE Birmingham June 2004
Ref 17 Jackson Grace E. (2005) Rethinking Psychiatric Drugs: A Guide for Informed Consent. Bloomington, IN: Author House.
Ref18 Reisner I, et al, (1996) http://www.ncbi.nlm.nih.gov/pubmed/8861609
Ref 19 Mehlman P, et al (1990) http://www.ncbi.nlm.nih.gov/pubmed/7522411
Ref 20 Brown GL & Linnoila MI (1990) http://www.ncbi.nlm.nih.gov/pubmed/1691169
Ref 21 Muller JL et al (2004) http://www.ncbi.nlm.nih.gov/pubmed/15570500
Ref 22 Odagaki (2009) http://www.benthamscience.com/cds/samples/cds4-1/0013CDS.pdf
Ref 23 Breggin (2003/4) http://www.breggin.com/31-49.pdf
Ref 24 Pert CB. Ph.D., (2001) http://ecommerce.drugawareness.org/Ribbon/SSRIMeds.html
Ref 25 Naveed Iqbal, MD, et al, (2007) http://www.cnsspectrums.com/aspx/articledetail.aspx?articleid=1262
Ref 26 Hall LM et al (1995) http://www.ncbi.nlm.nih.gov/pubmed/7543647
Ref 27 Grace Jackson MD (2009) Drug Induced Dementia. A Perfect Crime Bloomington, IN: Author House.
Ref 28 Siegel A, Bhatt S. (2007) http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2435345/
Ref 29 Stefan M. Brudzynski, et al (1990) http://www.ncbi.nlm.nih.gov/pubmed/2293258
Ref 30 Graeff FG. (1994) http://www.ncbi.nlm.nih.gov/pubmed/7916235
Ref 31 Imperato A. et al, (1993) “Evidence that neuroleptics increase striatal acetylcholine release through stimulation of dopamine D1 receptors” http://jpet.aspetjournals.org/content/266/2/557.abstract
Ref 32 Donald W. Black, Nancy C. Andreasen – Introductory Textbook of Psychiatry – (2011) 5th Edition p.544 American Psychiatric Publishing Inc.
Ref 33 Kasantikul D, Kanchanatawan B, (2006) http://www.ncbi.nlm.nih.gov/pubmed/17214072
Ref 34 Tanya C. Warwick, et al, (2008)
http://www.nature.com/nrneurol/journal/v4/n3/full/ncpneuro0728.html
Ref 35 Davies et al, (2000) http://www.national-toxic-encephalopathy-foundation.org/oppest.pdf
Ref 36 Singh S, Sharma N. Neurological syndromes following organophosphate poisoning. Neurol India 2000;48:308. http://www.neurologyindia.com/text.asp?2000/48/4/308/1510
Ref 37 Trends in prescriptions and costs of drugs for mental disorders in England, 1998–2010 Stephen Ilyas and Joanna Moncrieff (2012)
http://bjp.rcpsych.org/content/early/2012/03/10/bjp.bp.111.104257.abstract
Ref 38 NHS The Information Centre for Health and Social Care “Copyright © 2012, Re-used with the permission of the Health and Social Care Information Centre. www.ic.nhs.uk
Ref 39 Genelex http://www.healthanddna.com/healthcare-professional/dosing-recommendations.html
Ref 40 Genelex http://www.healthanddna.com/healthcare-professional/p450-2d6-genotyping.html
Ref 43 Todesco et al (2003) http://www.ncbi.nlm.nih.gov/pubmed/12851801
Ref 44 Asian PM for 2D6 Cozza et al 2003 and Richelson 1997 in Clinical Manual of Geriatric Psychopharmacology By Sandra A. Jacobson, Ronald W. Pies, Ira R. Katz Publisher: American Psychiatric Press Inc.; 1 edition (30 Jan 2007) Page 44 & 45
Ref 45 Joan Arehart-Treichel (2005)
http://pnhw.psychiatryonline.org/content/40/10/33.1.full
Ref 46 Lucire Y, Crotty C, (2011)
Ref 47 Bradford LD, Kirlin WG. (1998). http://www.ncbi.nlm.nih.gov/pubmed/11281961
Ref 48 Benny K. Abraham, C. Adithan (2001) http://medind.nic.in/ibi/t01/i3/ibit01i3p147.pdf
Ref 49 Genelex http://www.healthanddna.com/healthcare-professional/p450-2c19-genotyping.html
Ref 50 APRIL, Adverse Psychiatric Reactions Information Link http://www.april.org.uk/main/index.php?uid=269
Ref 51 Mental Health Foundation – Black and Minority Ethnic Communities
http://www.mentalhealth.org.uk/help-information/mental-health-a-z/B/BME-communities/
Ref 52 Stephen Pereira et al, (2006)
http://journals.cambridge.org/action/displayAbstract?fromPage=online&aid=651260
Ref 53 Anthony Feinstein and Frank Holloway(2002)
http://isp.sagepub.com/content/48/1/38.short
Ref 54 Len Bower (2008)
http://www.kcl.ac.uk/iop/depts/hspr/research/ciemh/mhn/projects/litreview/LitRevPICU.pdf
Ref 55 Community Care For everyone in social care “Mental Health Act detentions rise sharply for BME groups”
http://www.communitycare.co.uk/Articles/25/11/2009/113253/mental-health-act-detentions-rise-sharply-for-bme-groups.htm
Ref 56 National Mental Health Development Unit. BME Groups and Mental Health – Presentation and Evidence to the Centre for Social Justice Mental Health Review 18 October 2010. www.nmhdu.org.uk/silo/files/bme-groups-and-mental-health-.doc
Ref 57 Violence: The Short-Term Management of Disturbed/Violent Behaviour in Psychiatric In-patients and Emergency Departments Guideline, Appendix 1: Ethnicity review evidence tables. p.447 http://www.rcn.org.uk/__data/assets/pdf_file/0003/109812/003017_appendices.pdf










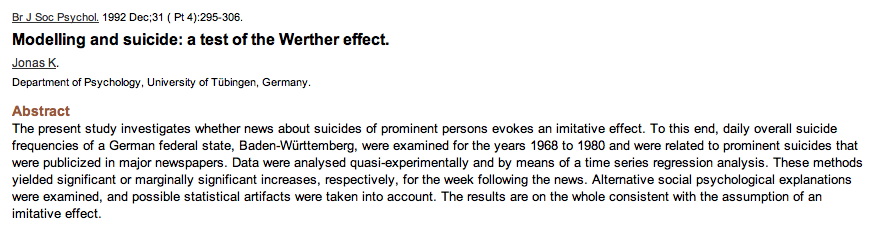
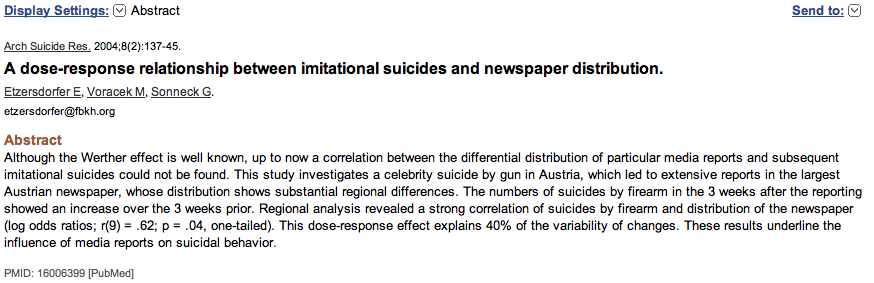


 I media sono complici di massacri
I media sono complici di massacri




























{kind=link}
{kind=link}
Devi effettuare l'accesso per postare un commento.